
Common errors identified in telemedicine billing
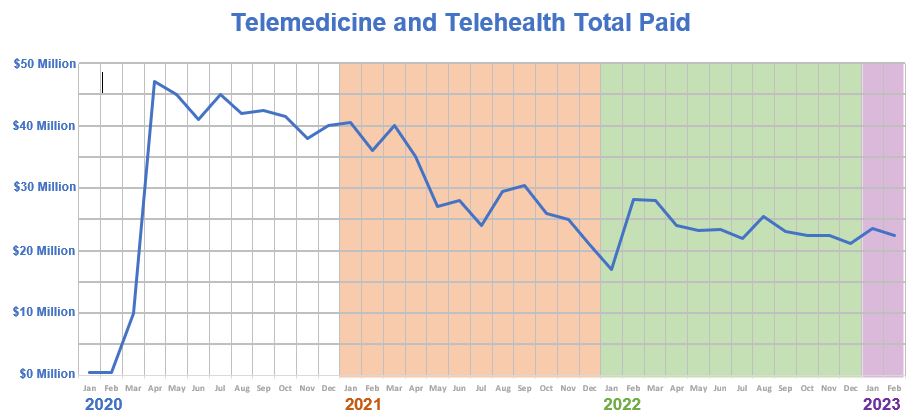
Physicians continue to use telemedicine at levels far above those used prior to the COVID-19 pandemic. Reimbursement for telemedicine and telehealth averaged less than $800,000 per month in 2019. By April 2020, Medicaid payments for virtual services jumped to $43 million. In 2023, average monthly spending has come down, but only to approximately $20 million.
Because of the increased risk for fraud as the technology was rapidly adopted, the OIG ramped up efforts to identify areas vulnerable to waste or wrongdoing. The OIG collaborated with providers and MCOs to identify dozens of potential issues and develop strategies to mitigate those risks.
The OIG can look across a variety of claims data for the entire state to identify trends and then focus on prevention and education. Billing patterns for these issues were identified during COVID as indicators of wasteful errors or possible suspicious activity. As telemedicine appears to be here to stay, these are some issues to watch for:
- Billing for multiple telemedicine or telehealth services on the same client in a short period of time, such as one month or even one day. This includes physicians calling patients as a “follow up” within the same week as a telemedicine visit and billing an evaluation and management (E&M) code; physicians performing telemedicine visits, then an in-person visit, with a modifier 25 (separately identifiable service) for the same diagnosis; and physicians calling patients they had not recently seen and who had not requested an appointment to “check up” on them and billing an E&M code.
- Impossible hours. Using timed procedure codes, providers are flagged if they bill for more than 24 hours in a day. There are situations in which telehealth services can be legitimately billed by a single provider in excess of 24 hours per day, such as services being rendered by assistants. If this is the case, it is taken into consideration. Providers should review each MCO’s policy since coding modifiers for this situation will vary by insurer.
- Telephone-only services. Billing more than one E&M code a day, with a modifier 25, on a patient would lead to improper reimbursement. E&M services cannot be billed if the physician determines an in-person or video telemedicine visit is required within 24 hours or the next available appointment time, as the services rendered via telephone will be considered part of the office or video visit. If a call follows an office visit within seven days for the same diagnosis, the telephone call is considered part of the previous visit and cannot be billed separately.
- Billing for Excess Time. The OIG audits examined teleservices claims paid for E&M with add-on psychotherapy services. The audits discovered clinics billing for more time than was spent with clients for the psychotherapy services, as evidenced by the time recorded in the medical records and by their telemedicine platforms. Providers are encouraged to implement processes to ensure that claims for services billed as time-based CPT codes are based on the actual length of services provided.